CLINICAL CASES
DISCOVER OUR SELECTION OF
CLINICAL CASES

SINGLE TOOTH RESTORATION IN A PATIENT WITH RISK FACTORS
Tooth 35 was extracted. 8 weeks later, a symbionic tooth was placed. 4.5 years post-insertion, the site showed stable, healthy soft tissue and shallow probing depths.

SINGLE TOOTH RESTORATION WITH AN INDIVIDUALIZED SYMBIONIC TOOTH
A failing restoration (45–47) was removed, and a symbionic tooth was placed at site 46. All sites received single crowns. Six years post-op, site 46 showed healthy soft tissue.

IMMEDIATE PLACEMENT OF SYMBIONIC TEETH IN THE ESTHETIC ZONE
Failing restorations of teeth 11 and 21 were removed and the tooth roots extracted. Two symbionic teeth were immediately placed and later restored with single crowns.
SINGLE TOOTH RESTORATION IN A PATIENT WITH RISK FACTORS
Tooth 35 was extracted. 8 weeks later, a symbionic tooth was placed. 4.5 years post-insertion, the site showed stable, healthy soft tissue and shallow probing depths.
SINGLE TOOTH RESTORATION WITH AN INDIVIDUALIZED SYMBIONIC TOOTH
A failing restoration (45–47) was removed, and a symbionic tooth was placed at site 46. All sites received single crowns. Six years post-op, site 46 showed healthy soft tissue.
IMMEDIATE PLACEMENT OF SYMBIONIC TEETH IN THE ESTHETIC ZONE
Failing restorations of teeth 11 and 21 were removed and the tooth roots extracted. Two symbionic teeth were immediately placed and later restored with single crowns.
SINGLE TOOTH RESTORATION IN A PATIENT WITH RISK FACTORS

Dr. Roland Glauser, Zurich, Switzerland

2 weeks post-op: nonirritated soft tissue

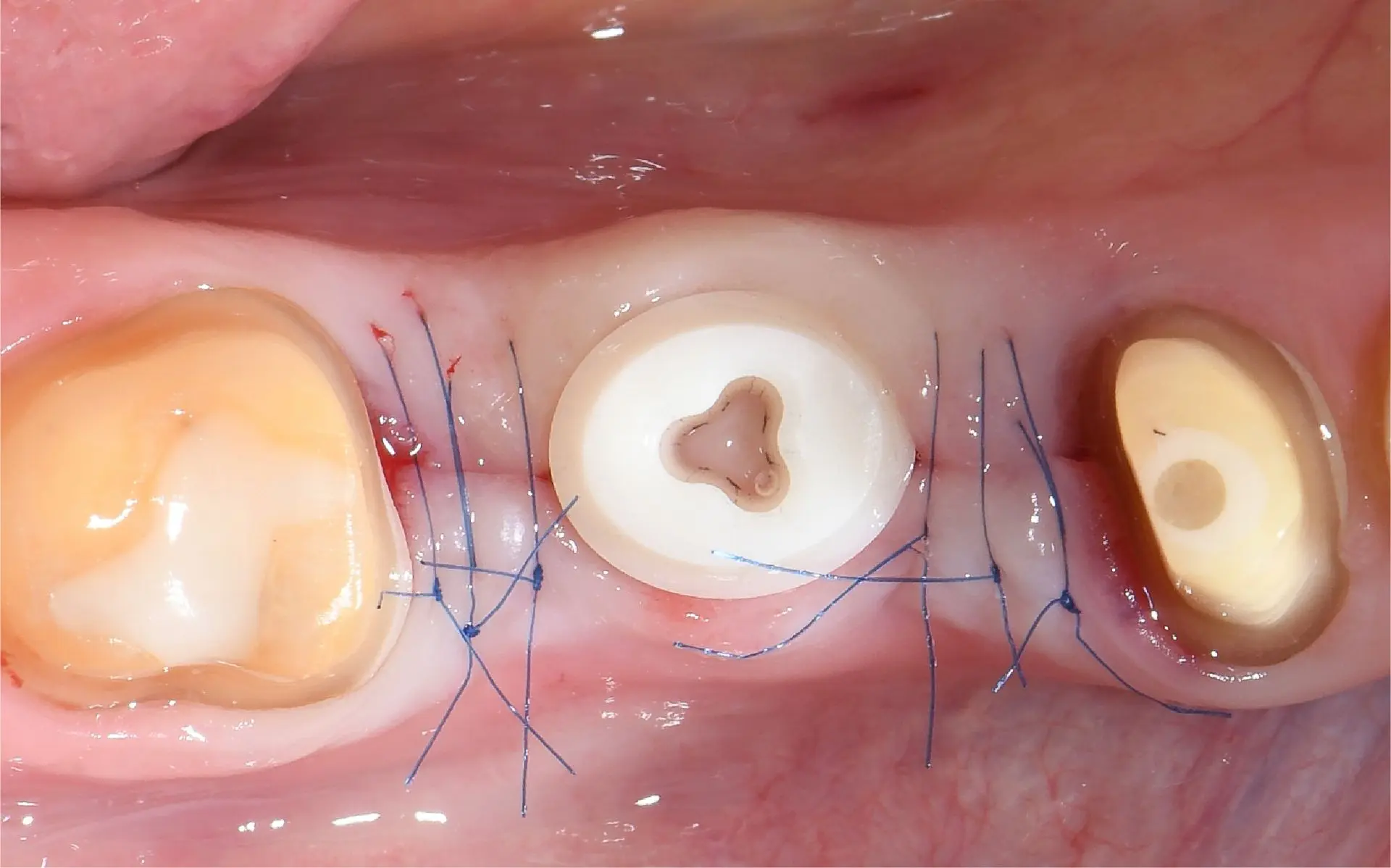
5 days post-op: stage-appropriate healing

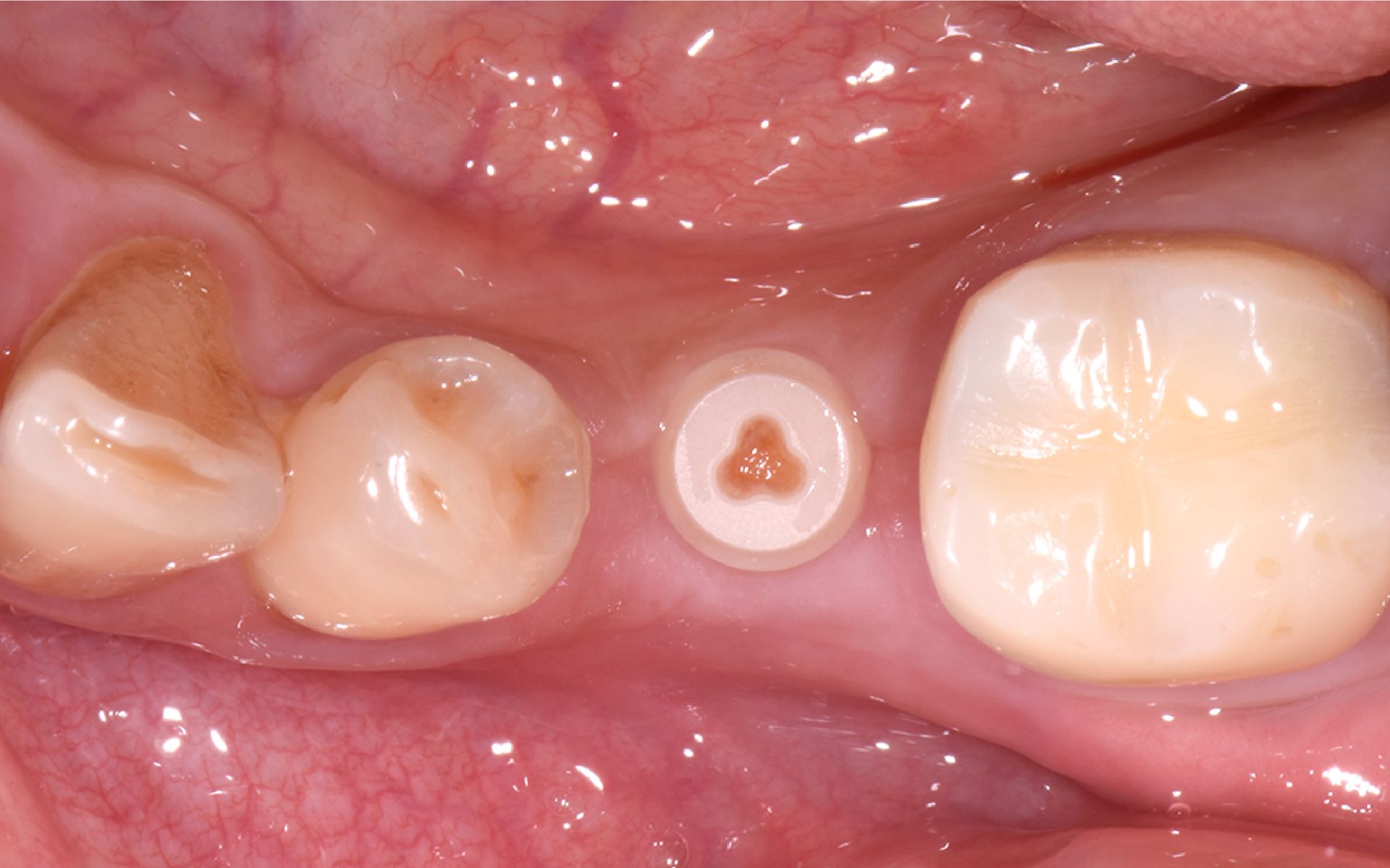
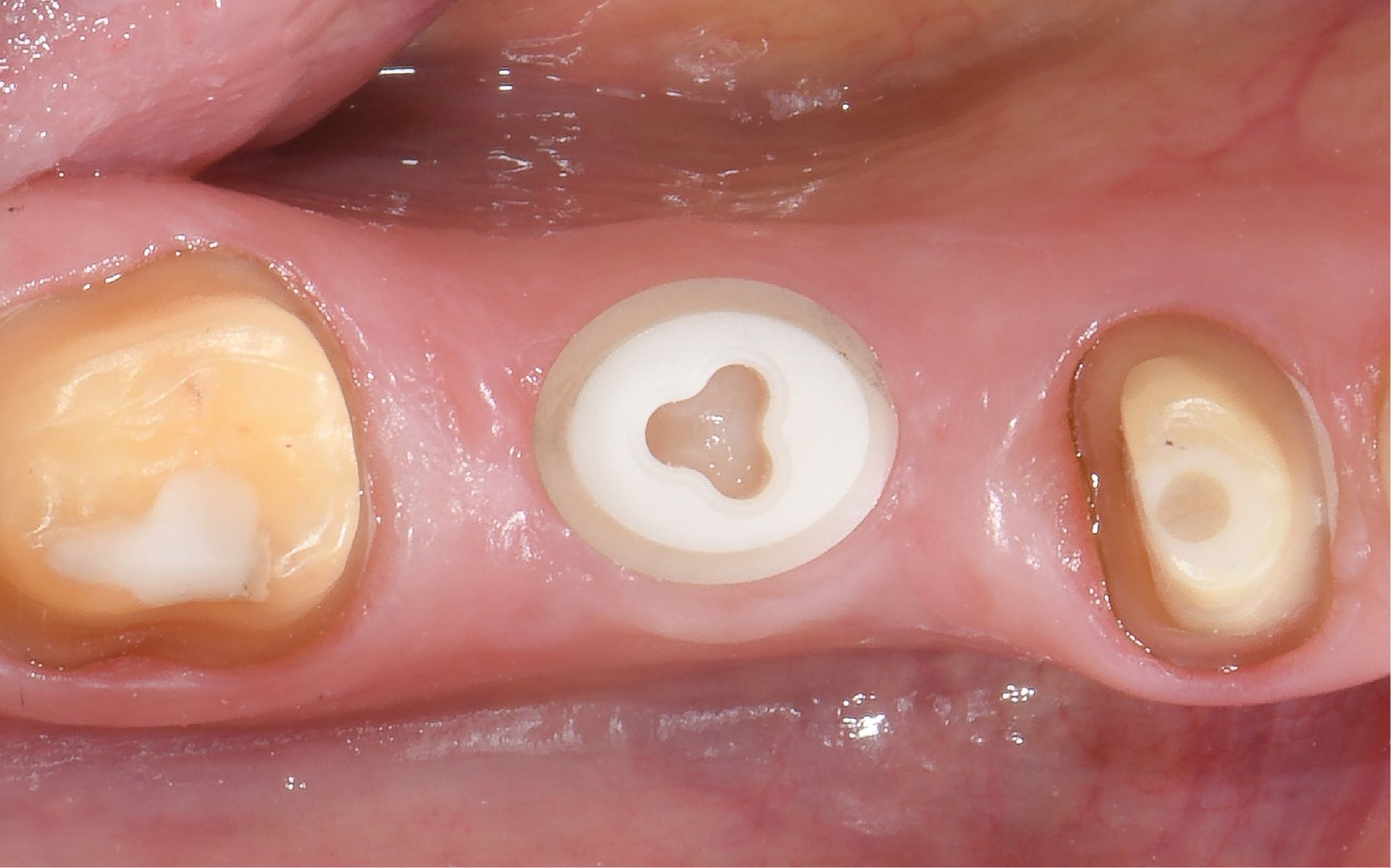
Situation after insertion

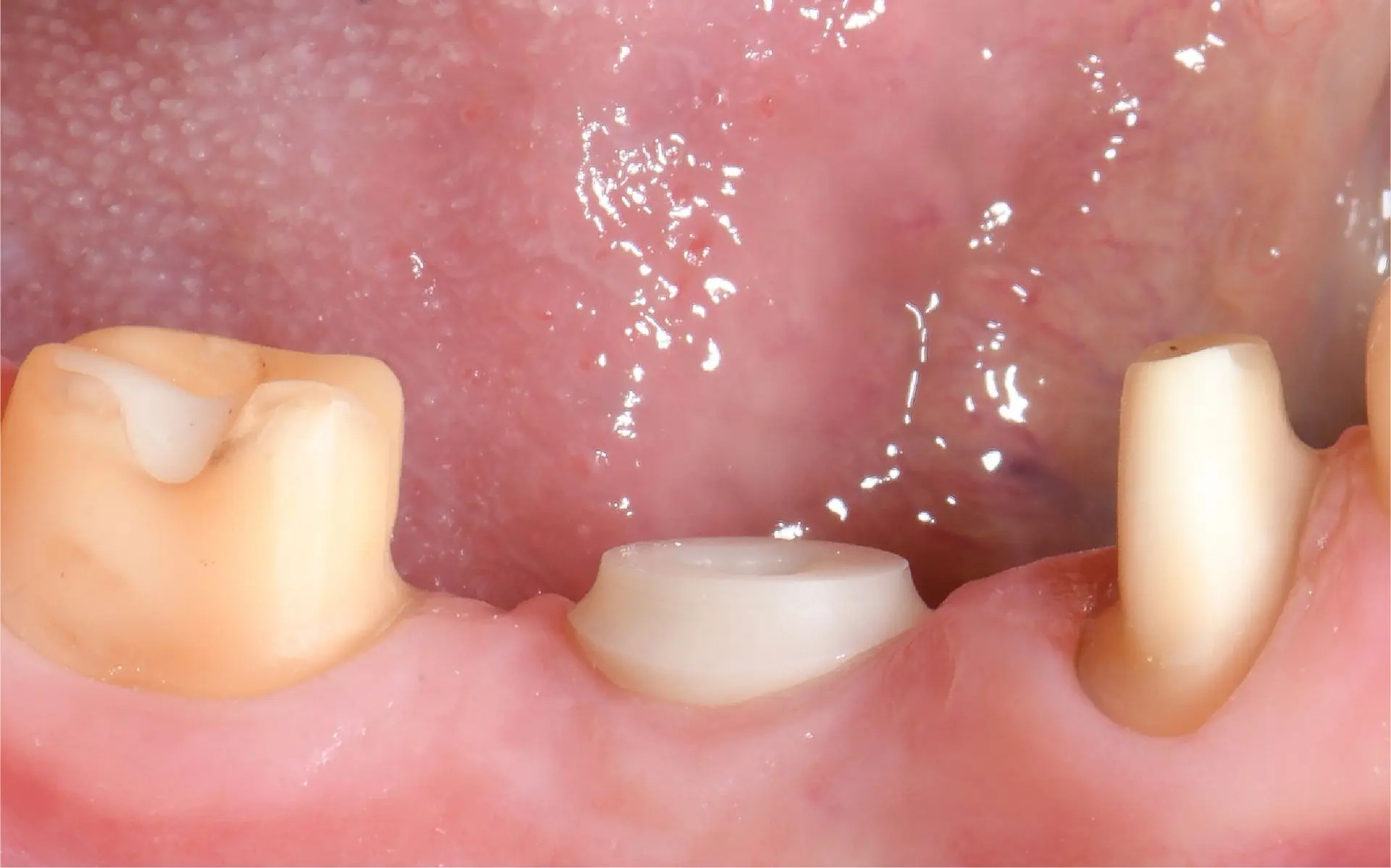
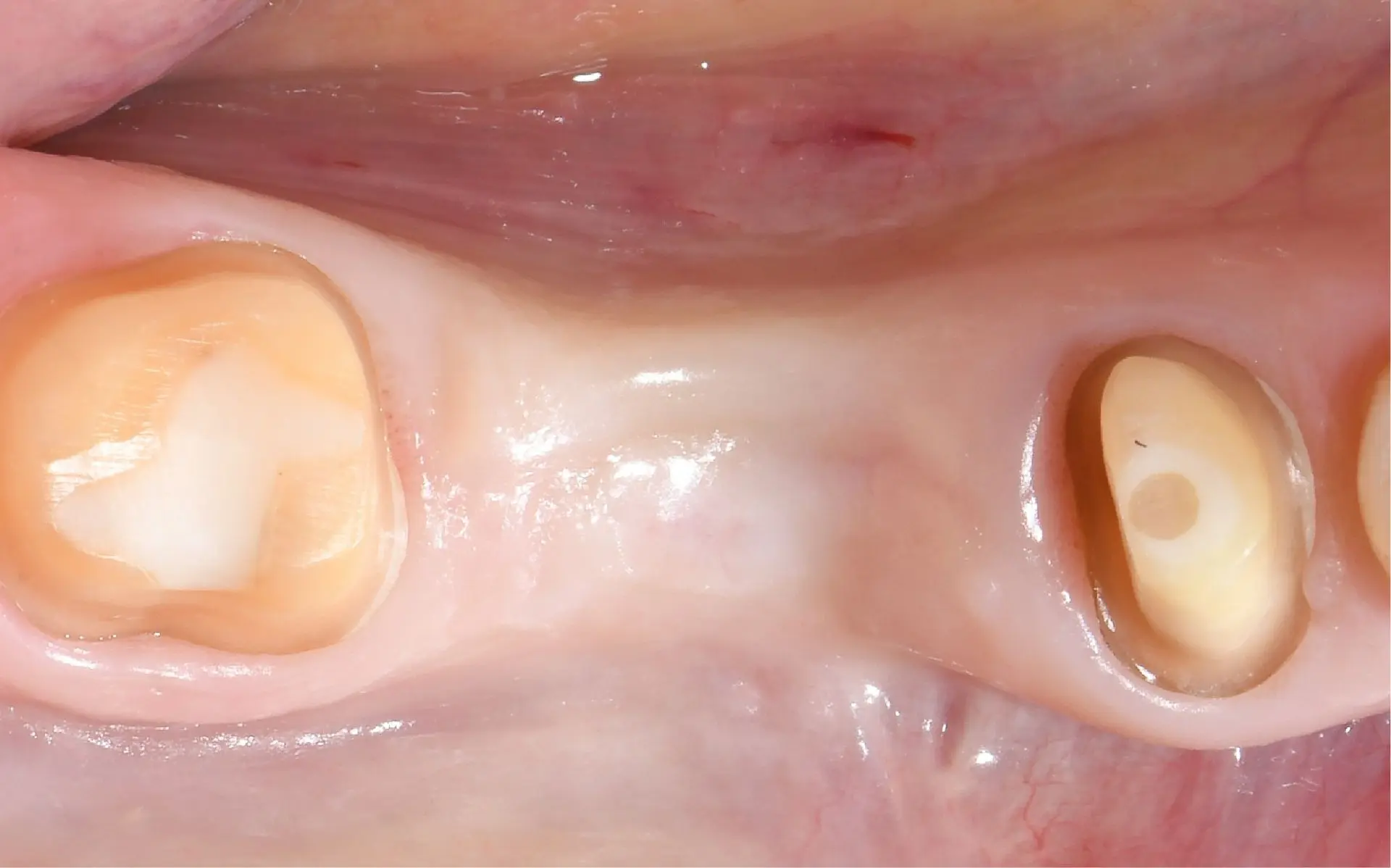
3 months after tooth extraction, before insertion
Dr. Roland Glauser
Zurich, Switzerland
Patient:
Male, 48 years old
Time of surgery:
2021
Follow-up period:
4.5 years
2 weeks post-op: nonirritated soft tissue
5 days post-op: stage-appropriate healing
Situation after insertion
3 months after tooth extraction, before insertion
SINGLE TOOTH RESTORATION IN A PATIENT WITH RISK FACTORS

4.5 years post-op: healthy soft tissue, shallow probing depths

3 years post-op: healthy and stable soft tissue
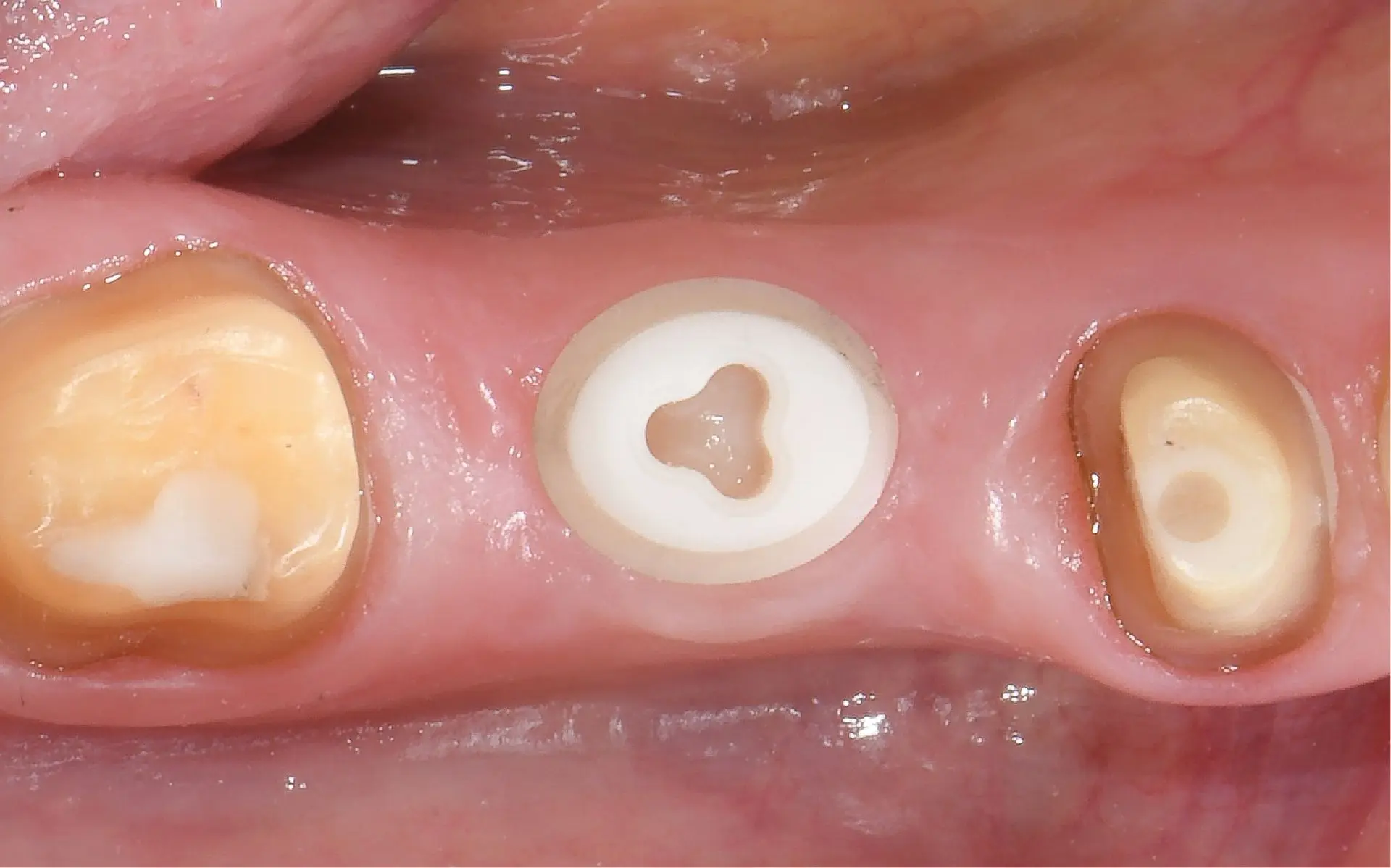
3 months post-op, before prosthetic restoration

6 weeks post-op: nonirritated soft tissue
4.5 years post-op: healthy soft tissue, shallow probing depths
3 years post-op: healthy and stable soft tissue
3 months post-op, before prosthetic restoration
6 weeks post-op: nonirritated soft tissue
Clinical situation
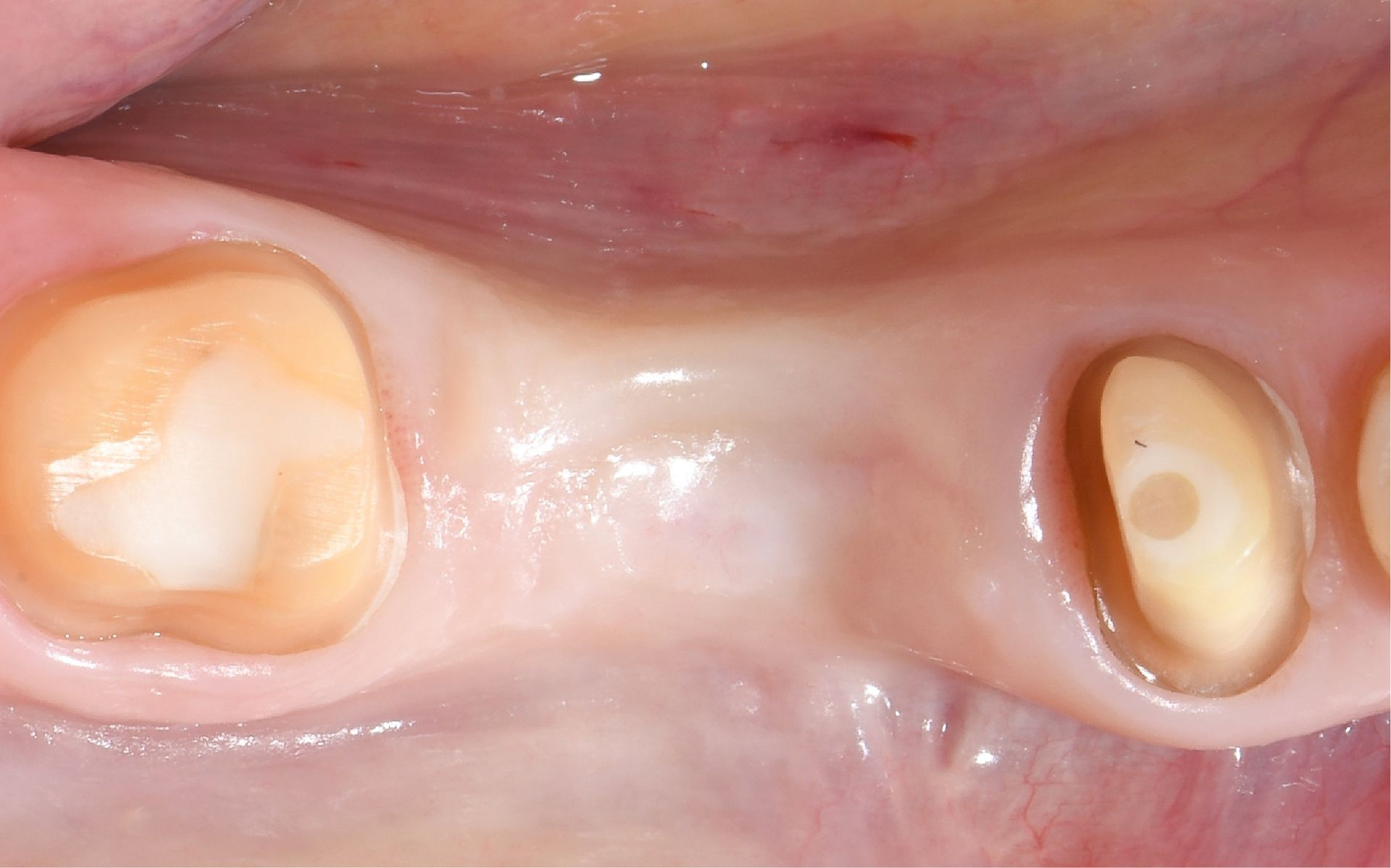
Tooth gap in region #35 following extraction elsewhere due to deep caries and acute pulpitis. The patient presented to the author’s practice eight weeks later requesting a fixed restoration. Slight horizontal ridge collapse. Soft-tissue thickness: 3 mm. Caries on adjacent crowned tooth #36.
Planned: symbionic tooth in region #35, treatment of tooth #36, and new single-tooth crowns on #35 and #36. Medical history included controlled Type 2 diabetes, smoking (20 cigarettes/ day), regular benzodiazepine use, and poor oral hygiene (BOP index: 38%).
Surgical solution
Modified mini-roll flap mobilized. Osteotomy prepared per protocol for D3 bone. Symbionic tooth inserted in region #35 at low speed with final torque of 11 Ncm.
Restorative solution
Glass fiber post cemented and prepared 3 months post-op. Full-arch impression taken. Partially veneered, individually characterized zirconia crowns cemented on symbionic tooth #35 and natural tooth #36.
Outcome
The follow-up after 4.5 years revealed a situation comparable to that of a healthy natural tooth, marked by healthy and stable soft tissue and shallow probing depths (Fig. 8).
Clinical situation
Tooth gap in region #35 following extraction elsewhere due to deep caries and acute pulpitis. The patient presented to the author’s practice eight weeks later requesting a fixed restoration. Slight horizontal ridge collapse. Soft-tissue thickness: 3 mm. Caries on adjacent crowned tooth #36.
Planned: symbionic tooth in region #35, treatment of tooth #36, and new single-tooth crowns on #35 and #36. Medical history included controlled Type 2 diabetes, smoking (20 cigarettes/ day), regular benzodiazepine use, and poor oral hygiene (BOP index: 38%).
Surgical solution
Modified mini-roll flap mobilized. Osteotomy prepared per protocol for D3 bone. Symbionic tooth inserted in region #35 at low speed with final torque of 11 Ncm.
Restorative solution
Glass fiber post cemented and prepared 3 months post-op. Full-arch impression taken. Partially veneered, individually characterized zirconia crowns cemented on symbionic tooth #35 and natural tooth #36.
Outcome
The follow-up after 4.5 years revealed a situation comparable to that of a healthy natural tooth, marked by healthy and stable soft tissue and shallow probing depths (Fig. 8).

Dr. Sebastian Horvath
Jestetten, Germany
Patient:
Female, 54 years old
Time of surgery:
2019
Follow-up period:
6 years
3 months after insertion, before post bonding and preparation
3 months after insertion.
Situation after insertion
Initial situation.
SINGLE TOOTH RESTORATION WITH AN INDIVIDUALIZED SYMBIONIC TOOTH

6 years post-op: healthy and stable soft tissue.

3.5 years post-op: healthy and stable soft tissue.

Situation after delivery of final crowns.
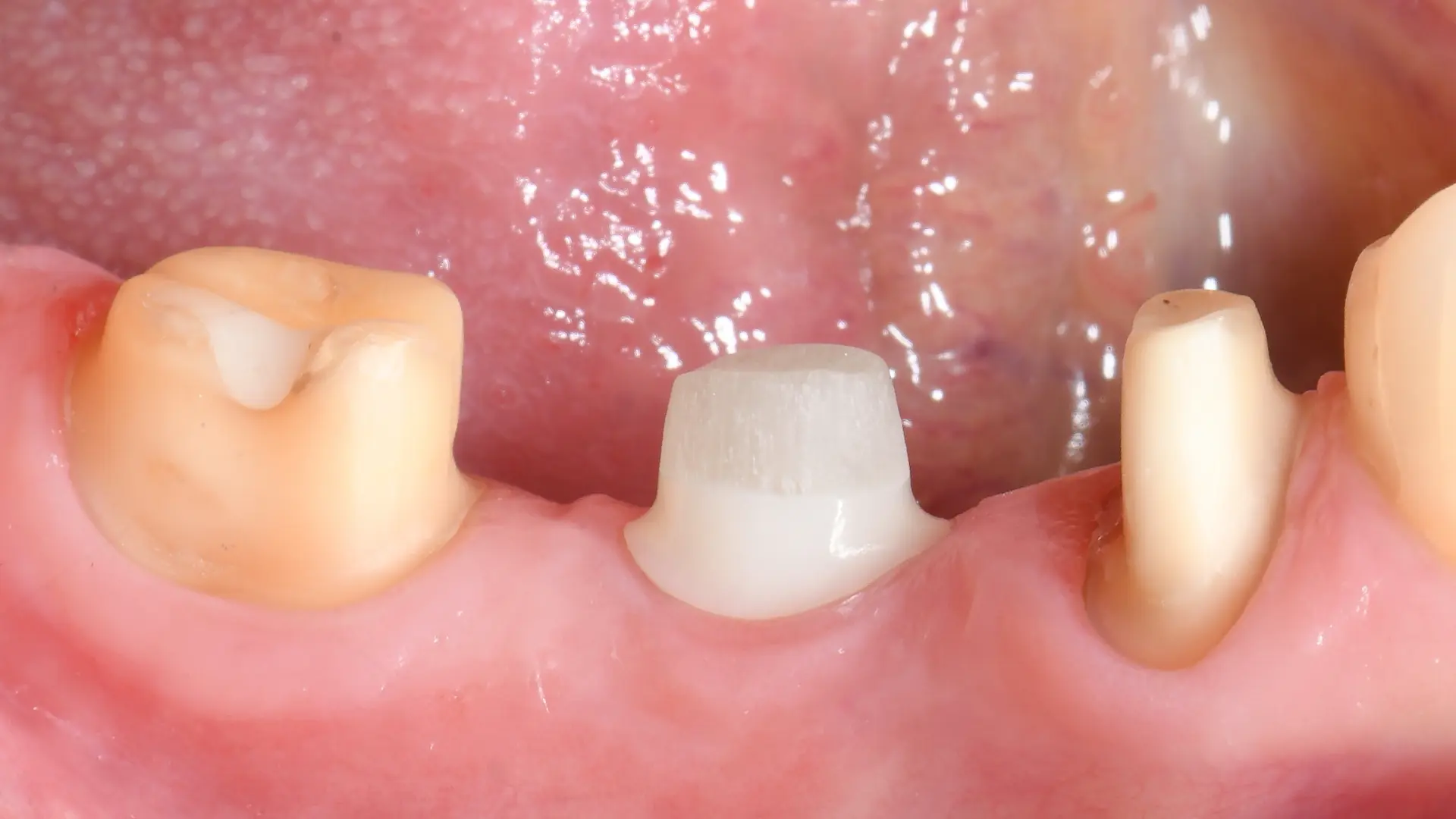
Situation after preparation of post and shoulder of symbionic tooth.
SINGLE TOOTH RESTORATION WITH AN INDIVIDUALIZED SYMBIONIC TOOTH

Dr. Sebastian Horvath, Jestetten, Germany

3 months after insertion, before post bonding and preparation.
3 months after insertion.
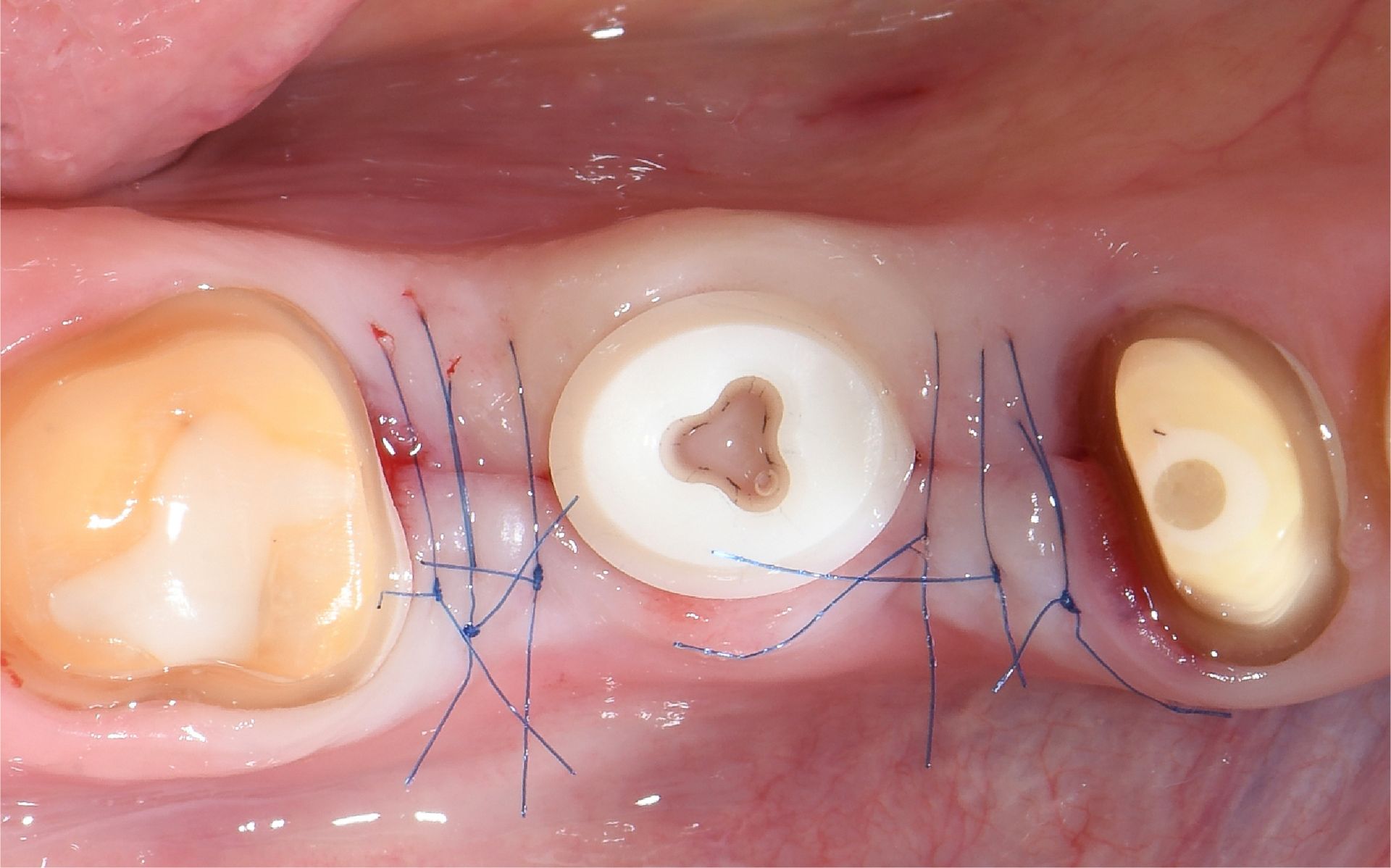
Situation after insertion
Initial situation.

6 years post-op: healthy and stable soft tissue.

3.5 years post-op: healthy and stable soft tissue.

Situation after delivery of final crowns.
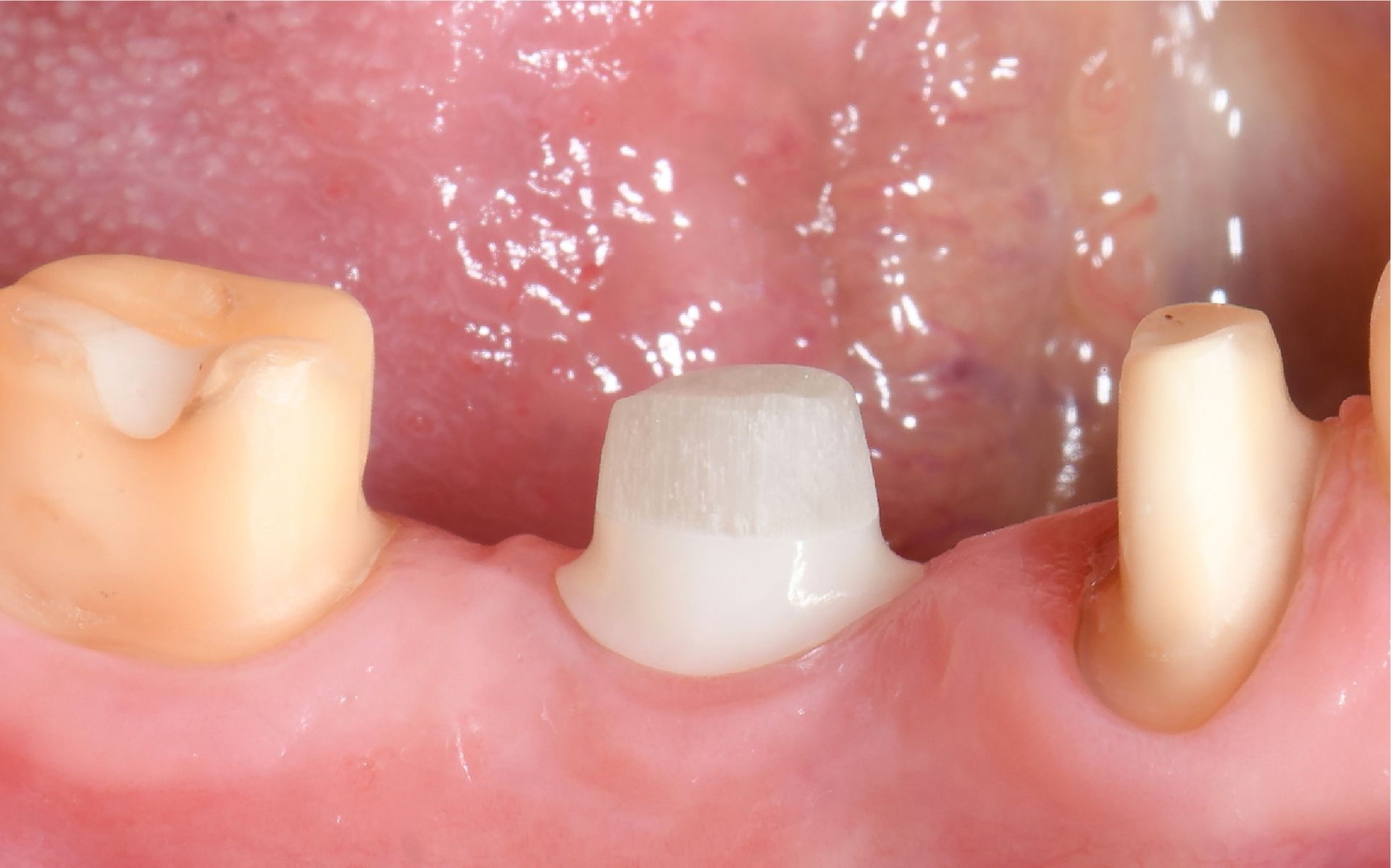
Situation after preparation of post and shoulder of symbionic tooth.
Clinical situation
Old restoration spanning regions #45–47, placed about 20 years ago, required replacement. Tooth gap in region #46. Tooth #45 endodontically treated. Increased sensitivity of tooth #47 due to ill-fitting margins. Planned: Symbionic tooth in region #46, single-tooth crowns on #45, #46, and #47.
Surgical solution
Full-thickness flap elevated in region #46. Surgical guide positioned. Osteotomy prepared at 600 RPM according to the manufacturer’s protocol for D2 bone. Symbionic tooth inserted to a moderate final torque of 30 Ncm. 3C™ Connection sealed with Teflon tape.
Restorative solution
3 months post-op: Glass fiber post bonded to the 3C™ Connection and prepared with high-speed diamond burs of varying grit. Shoulder of symbionic tooth prepared for optimal emergence profile. Full arch including prepared post scanned. Monolithic zirconia crowns fabricated and cemented in subsequent session.
Outcome
Compared to the situation after definitive restoration (Fig. 6), the soft tissue around the symbionic tooth #46 remains healthy and stable after 6 years, whereas the natural teeth #45 and #47 show signs of gingival recession (Fig. 8).
IMMEDIATE PLACEMENT OF SYMBIONIC TEETH IN THE ESTHETIC ZONE

Dr. Fabio Rossi, Dr. Filippo Battelli
Studio Dentisitco. Bologna, Rimini, Italy

2 months post-op: healthy soft tissue.

4 weeks post-op: nonirritated soft tissue.
1 week post-op: stage-appropriate healing.
3 days post-op: stage-appropriate healing.
Clinical situation
Old restoration spanning regions #45–47, placed about 20 years ago, required replacement. Tooth gap in region #46. Tooth #45 endodontically treated. Increased sensitivity of tooth #47 due to ill-fitting margins. Planned: Symbionic tooth in region #46, single-tooth crowns on #45, #46, and #47.
Surgical solution
Full-thickness flap elevated in region #46. Surgical guide positioned. Osteotomy prepared at 600 RPM according to the manufacturer’s protocol for D2 bone. Symbionic tooth inserted to a moderate final torque of 30 Ncm. 3C™ Connection sealed with Teflon tape.
Restorative solution
3 months post-op: Glass fiber post bonded to the 3C™ Connection and prepared with high-speed diamond burs of varying grit. Shoulder of symbionic tooth prepared for optimal emergence profile. Full arch including prepared post scanned. Monolithic zirconia crowns fabricated and cemented in subsequent session.
Outcome
Compared to the situation after definitive restoration (Fig. 6), the soft tissue around the symbionic tooth #46 remains healthy and stable after 6 years, whereas the natural teeth #45 and #47 show signs of gingival recession (Fig. 8).
IMMEDIATE PLACEMENT OF SYMBIONIC TEETH IN THE ESTHETIC ZONE
Dr. Fabio Rossi
Dr. Filippo Battelli
Studio Dentisitco
Bologna, Rimini
Italy
Patient:
Female, 55 years old
Time of surgery:
2021
Follow-up period:
3 years
2 months post-op: healthy soft tissue.
4 weeks post-op: nonirritated soft tissue.
1 week post-op: stage-appropriate healing.
3 days post-op: stage-appropriate healing.

6 months after delivery of final crowns: healthy soft tissue.

15 days after delivery of final crowns: healthy soft tissue.

1 week after delivery of final crowns: healthy soft tissue.

Situation after delivery of final crowns (3 months post-op).
6 months after delivery of final crowns: healthy soft tissue.
15 days after delivery of final crowns: healthy soft tissue.
1 week after delivery of final crowns: healthy soft tissue.
Situation after delivery of final crowns (3 months post-op).

3 years after delivery of final crowns: healthy soft tissue.

2 years after delivery of final crowns: healthy soft tissue.
3 years after delivery of final crowns: healthy soft tissue.
2 years after delivery of final crowns: healthy soft tissue.
Clinical situation
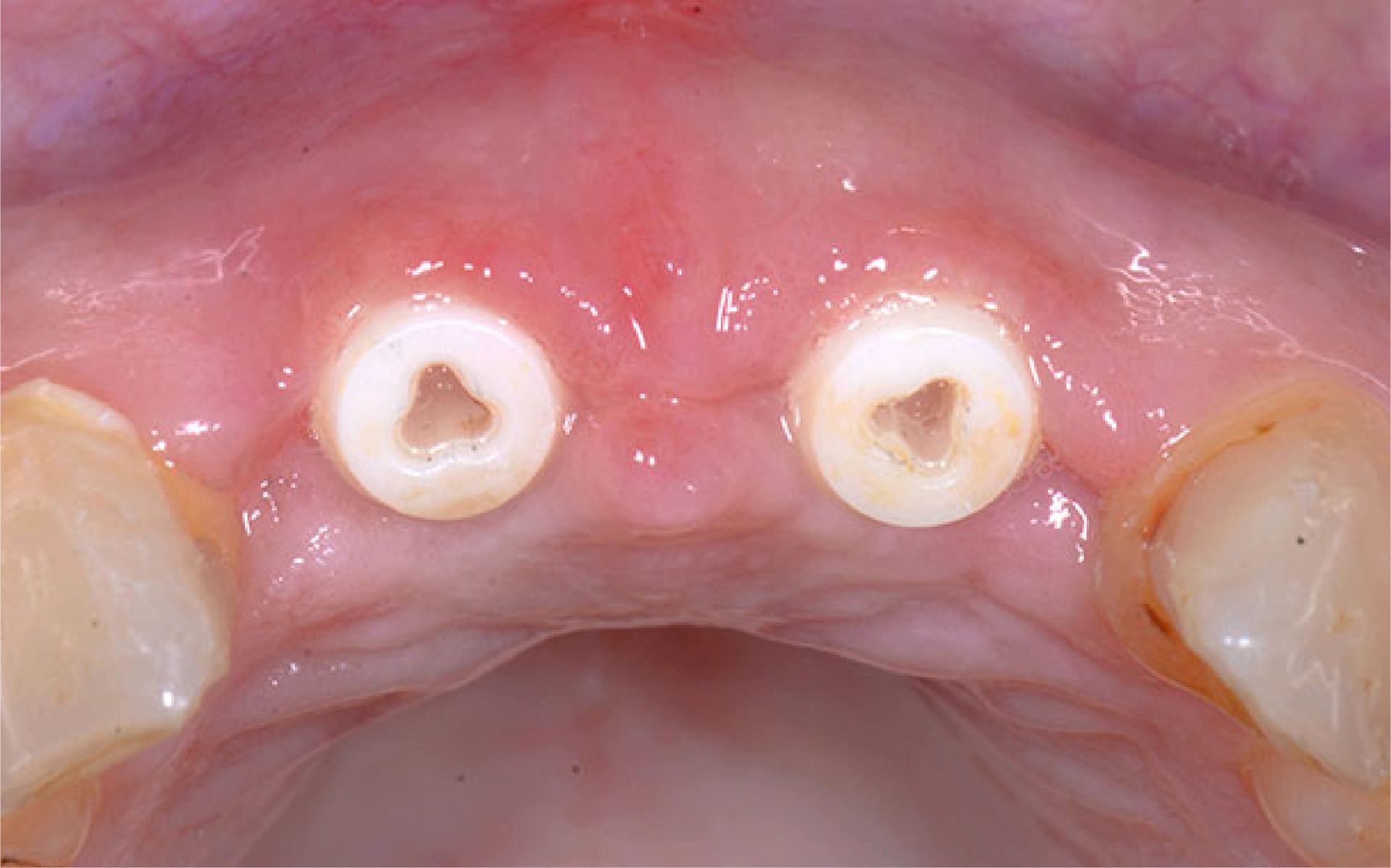
Failing post-and-core restorations of teeth #11 and #21 required replacement. The patient requested a fixed tooth replacement solution. Planned treatment included removal of the failing restorations, extraction of the remaining tooth roots, immediate placement of two Patent™ Symbionic Teeth, and restoration with final crowns following successful integration.
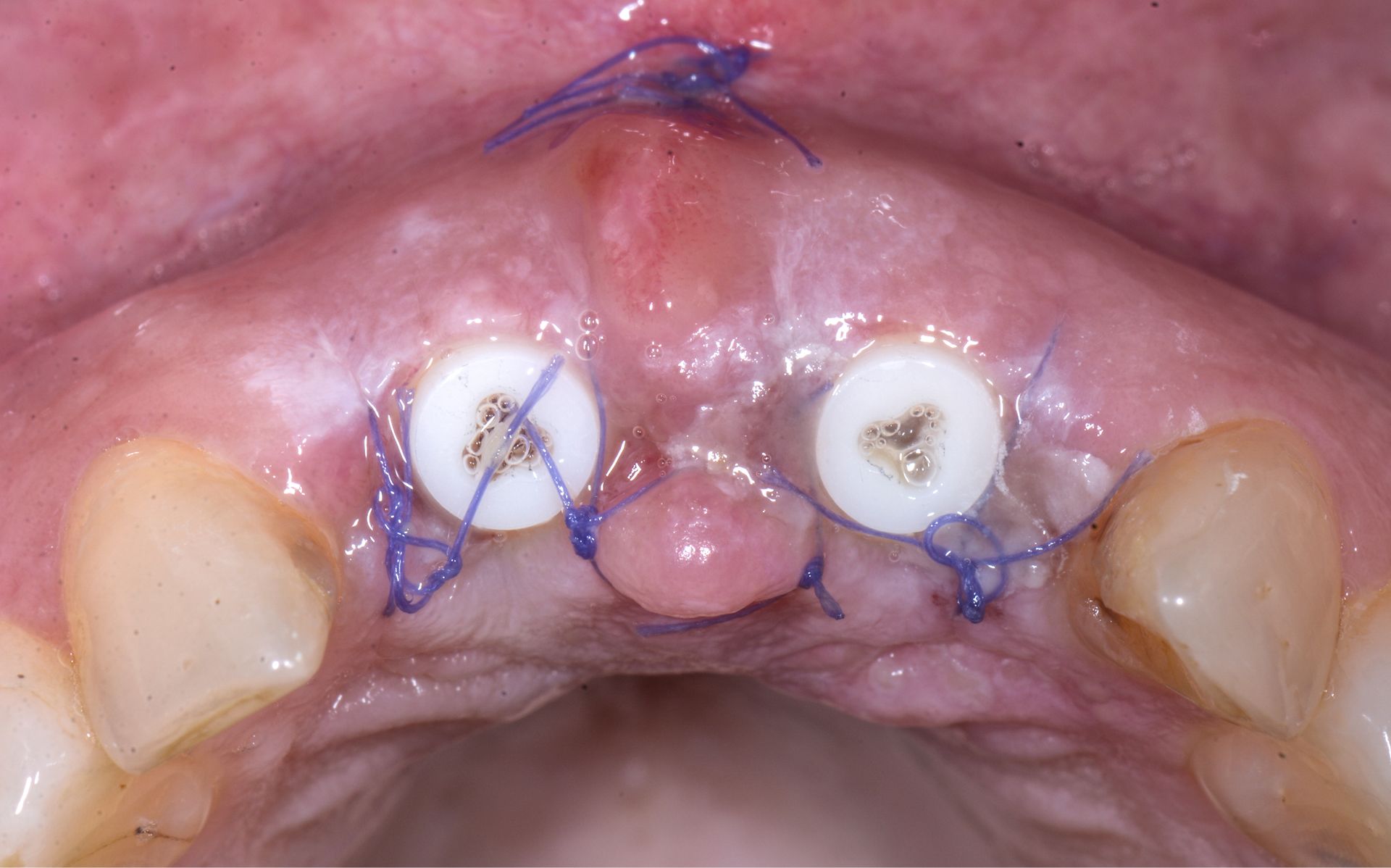
Surgical solution
Vestibular incisions were made in regions #11 and #21. The old restorations were removed, and the tooth roots were extracted. The alveoli were curetted. A surgical guide was placed, and osteotomies were prepared according to the manufacturer’s protocol for D3 bone at 600 RPM. Symbionic Teeth were
inserted to moderate final torque.
Restorative solution
Glass fiber posts were cemented and prepared 2 months post-surgery. A digital impression of the entire arch, including the prepared posts, was taken using an intraoral scanner. The posts were isolated with glycerin oil, and provisional crowns were cemented using a temporary cement mixture.
Final crowns were delivered after 3 months of healing.
Outcome
At the 3-year follow-up (Fig. 10), the situation is characterized by healthy and stable soft tissue, resulting in excellent esthetics.
Clinical situation
Failing post-and-core restorations of teeth #11 and #21 required replacement. The patient requested a fixed tooth replacement solution. Planned treatment included removal of the failing restorations, extraction of the remaining tooth roots, immediate placement of two Patent™ Symbionic Teeth, and restoration with final crowns following successful integration.
Surgical solution
Vestibular incisions were made in regions #11 and #21. The old restorations were removed, and the tooth roots were extracted. The alveoli were curetted. A surgical guide was placed, and osteotomies were prepared according to the manufacturer’s protocol for D3 bone at 600 RPM. Symbionic Teeth were
inserted to moderate final torque.
Restorative solution
Glass fiber posts were cemented and prepared 2 months post-surgery. A digital impression of the entire arch, including the prepared posts, was taken using an intraoral scanner. The posts were isolated with glycerin oil, and provisional crowns were cemented using a temporary cement mixture.
Final crowns were delivered after 3 months of healing.
Outcome
At the 3-year follow-up (Fig. 10), the situation is characterized by healthy and stable soft tissue, resulting in excellent esthetics.